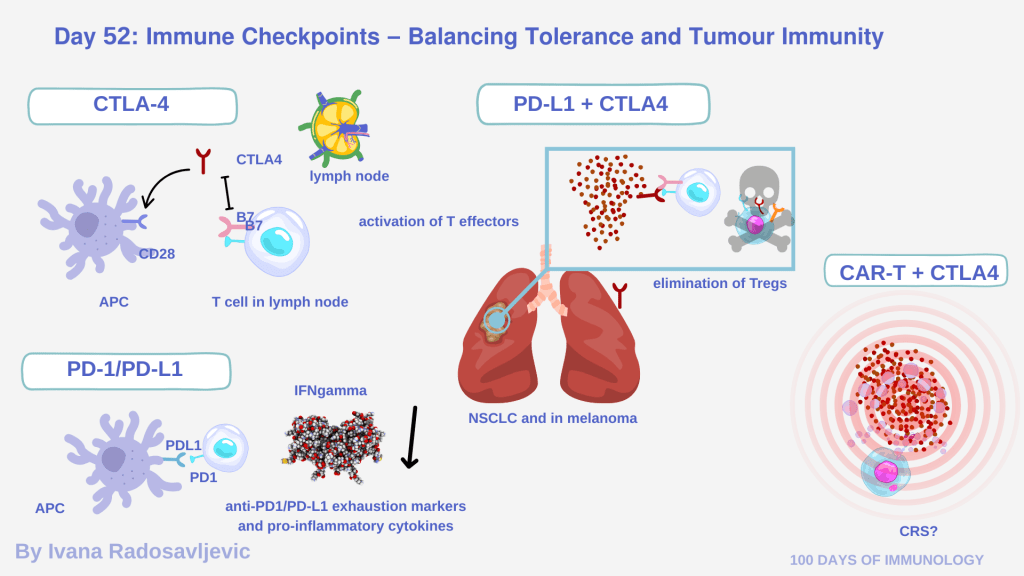
Immune checkpoint molecules such as 𝘊𝘛𝘓𝘈‐4 and 𝘗𝘋‐1 act as brakes on T-cell activation. CTLA-4 competes with CD28 for B7 ligands on antigen-presenting cells (APCs), limiting T-cell priming in lymph nodes. PD-1 is up-regulated on 𝘢𝘤𝘵𝘪𝘷𝘢𝘵𝘦𝘥/𝘦𝘹𝘩𝘢𝘶𝘴𝘵𝘦𝘥 𝘛 𝘤𝘦𝘭𝘭𝘴 in peripheral tissues and, upon binding PD-L1/PD-L2, inhibits proliferation, cytokine production and survival of effector T cells [2][5]. Therapies: Anti-CTLA-4 amplifies naïve-T-cell activation and may deplete regulatory T cells (Tregs) in the tumour micro-environment (TME), while anti-PD-1/PD-L1 primarily restores effector function of tumour-infiltrating exhausted T cells [3][11].
𝗠𝗲𝗰𝗵𝗮𝗻𝗶𝘀𝗺 𝗼𝗳 𝗔𝗰𝘁𝗶𝗼𝗻
CTLA-4 blockade enhances co-stimulation by CD28 and expands T-cell receptor (TCR) repertoire, supporting early immune activation [5].
PD-1/PD-L1 blockade relieves exhaustion-associated signals in T cells residing in the TME, increasing cytotoxicity and cytokine release (e.g., IFN-γ, TNF) [2].
𝗖𝗹𝗶𝗻𝗶𝗰𝗮𝗹 𝗜𝗻𝘀𝗶𝗴𝗵𝘁𝘀 & 𝗖𝗼𝗺𝗯𝗶𝗻𝗮𝘁𝗶𝗼𝗻𝘀
Combination therapy of anti-CTLA-4 plus anti-PD-1 shows clinical efficacy in some cancers (melanoma and NSCLC), with enhanced infiltration of effector T cells and elimination of Tregs. This dual blockade also increases the incidence and severity of immune-related adverse events (irAEs), such as colitis, hepatitis, etc. [1][4]
𝗦𝗽𝗲𝗰𝘂𝗹𝗮𝘁𝗶𝘃𝗲 𝗵𝘆𝗽𝗼𝘁𝗵𝗲𝘀𝗶𝘀:
Combining checkpoint inhibitors with CART cells appears promising – but a double sword – a joint blockade of PD-1/PD-L1, CTLA-4 and simultaneous CAR-T therapy might unleash an uncontrolled immune cascade, CRS. The key question remains: Is the immune system being released and overloaded, or is the tumor awakening the inflammatory molecules that drive immune escape? Emerging pre-clinical data suggest that persistent inflammation (driven by oncogenes) may establish immune suppressive niches, which then resist checkpoint plus CAR-T combination unless the TME is reprogrammed first [3]. The arguments are against CAR-T + anti-CTLA-4, since antibody acts on T cell priming, and that is not relevant for activated T cells.
𝗤𝘂𝗲𝘀𝘁𝗶𝗼𝗻 𝗳𝗼𝗿 𝘁𝗵𝗲 𝗮𝘂𝗱𝗶𝗲𝗻𝗰𝗲: Your thoughts on combining CAR-T therapy with dual checkpoint blockade – do the combined therapy benefits outweigh the potential toxicities?
Stay tuned for 𝗗𝗮𝘆 𝟱𝟯: 𝗔𝗱𝗼𝗽𝘁𝗶𝘃𝗲 𝗰𝗲𝗹𝗹 𝘁𝗵𝗲𝗿𝗮𝗽𝘆: 𝗲𝗺𝗽𝗼𝘄𝗲𝗿𝗶𝗻𝗴 𝘁𝗵𝗲 𝗶𝗺𝗺𝘂𝗻𝗲 𝗮𝗿𝗺𝘆
𝗥𝗲𝗳𝗲𝗿𝗲𝗻𝗰𝗲𝘀:
1. DOI:10.1007/s10147-019-01588-7
2. DOI: 10.1186/s13045-018-0578-4
3. DOI: 10.1186/s40164-019-0150-0
4. DOI: 10.15419/bmrat.v9i12.784
5. DOI: 10.3389/fimmu.2023.1264327
#100DaysOfImmunology #ImmuneCheckpoints #CancerImmunology #ImmunoOncology #PD1 #CTLA4 #CombinationTherapy #CAR_T #TumorMicroenvironment #irAEs
